

Peptide Calculator: Accurate Dosing Tool for Research in 2026
Stop guessing your peptide doses. Use our free peptide calculator to convert mg, mcg, and
The most counterintuitive fact in Epitalon work is this: the dose many researchers treat as standard may be far above the dose suggested by the original animal-to-human translation. A published analysis argues that the common 5 to 10 mg/day subcutaneous protocol conflicts with the biologically equivalent human extrapolation from the foundational rodent scale, which comes out closer to 0.5 to 1 mg/day (translational dosing analysis).
That gap matters. If a study is trying to map mechanism, define a threshold response, or compare cycle designs, starting too high can blur the signal. Epitalon is a small synthetic tetrapeptide, Ala-Glu-Asp-Gly, used in laboratory settings to investigate circadian regulation, melatonin biology, and cellular aging. It is not approved for human use outside limited regional contexts involving related compounds, so protocol design has to be tighter than the community norm. In practice, that means dose selection, route, preparation, storage, and material quality all matter as much as the peptide itself.
The biggest mistake in Epitalon protocol design is assuming that the most repeated dose is automatically the most rational dose. It often isn't. In this field, epitalon peptide dosage has split into two camps: a widely circulated high-dose convention and a lower-dose framework that tracks more closely with translational reasoning from the original animal work.
That split creates avoidable noise in experiments. If one lab runs a low-dose circadian study and another runs a higher-dose longevity cycle, they may both claim to be studying Epitalon while testing different biological intents. Dose isn't a housekeeping detail. It's part of the hypothesis.
Researchers usually inherit one of these assumptions:
Those aren't minor variations. They produce very different exposure conditions.
Practical rule: If the goal is to identify minimum effective exposure, a protocol that starts at the top of the community range answers the wrong question.
A disciplined Epitalon study usually starts with four design decisions:
Epitalon remains an experimental compound in most regulatory environments. That puts more weight on reproducibility, not less. The stronger the claim you want from a study, the tighter the dose logic has to be.
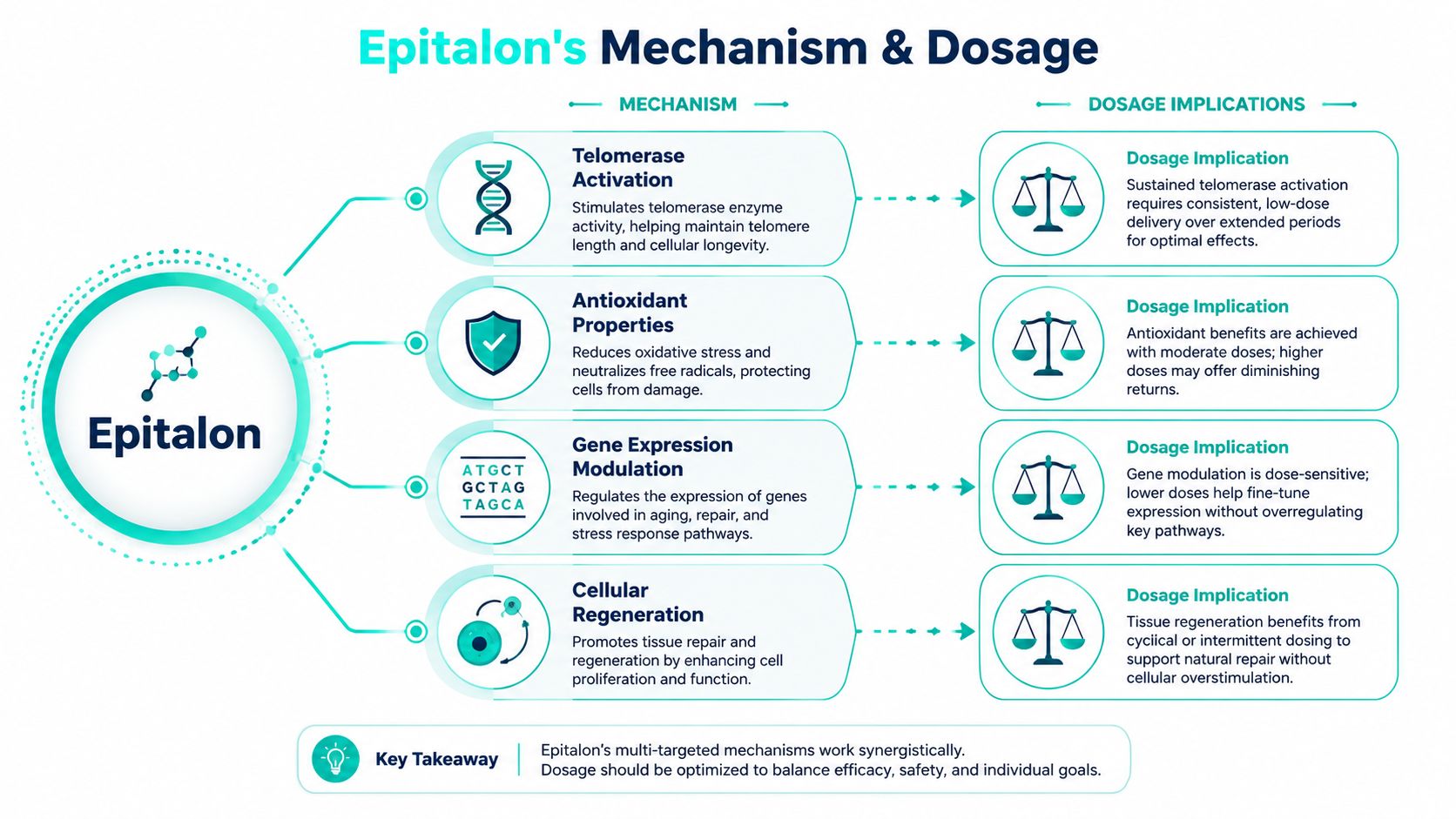
Dose selection makes more sense once you separate Epitalon's biological roles. Researchers often discuss it as one peptide with one anti-aging effect. Mechanistically, that framing is too blunt.
One side of Epitalon's activity concerns pineal signaling and melatonin regulation. The other concerns telomerase and longer-horizon cellular aging pathways. Those goals don't necessarily need the same exposure pattern.
Think of the melatonin effect as flipping a light switch. Once the relevant signaling threshold is reached, a measurable endocrine response may appear without pushing the dose much higher. Think of the telomere-related hypothesis as slowly charging a battery. The output is less immediate, more cumulative, and more dependent on how the experiment is structured over time.
That distinction explains why some researchers see the lower-dose range as biologically plausible, while others keep using the higher-dose community standard. They may be aiming at different phenomena but using the same label.
In practice, mechanism-driven dosing usually follows this logic:
A useful way to structure Epitalon studies is to ask one direct question: are you trying to prove that the peptide can produce an effect, or are you trying to identify the least exposure needed to produce it reproducibly? Those are different experiments.
The cleanest protocol is usually the one that can still detect a signal without overwhelming the system.
Another practical issue is concentration sensitivity. The translational analysis argues that Epitalon's bioactivity may be sensitive to threshold effects in pineal and immune pathways, which is one reason the difference between 0.5 to 1 mg/day and 5 to 10 mg/day shouldn't be treated as trivial. If a pathway saturates early, a larger dose may add exposure without adding clarity.
Researchers who skip this mechanistic distinction often overinterpret null results. A failed high-dose study doesn't necessarily disprove low-dose circadian utility. A positive low-dose melatonin response doesn't automatically validate a telomerase-focused protocol. The endpoint and the dose have to match.
The biggest dosing mistake in Epitalon research is treating the community standard as if it were the scientific baseline. It is not. Published human and translational material points to a much lower starting range for many experiments, while the commonly repeated 5 to 10 mg protocol appears to be a legacy convention carried forward across clinics, forums, and secondary writeups.
That distinction matters because dose selection changes the question your study is asking. A low-dose protocol tests whether Epitalon has measurable activity near the biologically extrapolated range. A high-dose protocol tests whether heavy exposure can force a signal in a broad longevity model. Those are different designs, and they should not be described as interchangeable.
Human-facing reports cited earlier in this article describe a measurable melatonin-related response at 0.5 mg/day with subcutaneous administration. That is the cleanest reason to take sub-milligram dosing seriously. It shows that detectable physiological activity does not require a 5 to 10 mg starting point.
Published translational analysis also matters here. The original animal work is commonly summarized in a way that, after human dose translation, lands closer to 0.5 to 1 mg/day rather than the community-standard 5 to 10 mg/day. That does not settle the question for every endpoint. It does establish that the lower range is scientifically grounded and should not be dismissed as underdosing.
The higher-dose protocol is easy to find in peptide communities and private longevity clinics. The usual pattern is 5 to 10 mg/day, often by subcutaneous injection, for 10 to 20 days per cycle, repeated once or twice per year. Researchers also encounter related historical protocols from Russian peptide practice using intramuscular schedules and adjacent glandular peptide products, which likely helped reinforce the idea that multi-milligram cycling was standard.
Protocol inheritance is common in this field. One group copies a clinic schedule. Another group copies a reseller guide. A third group repeats the same numbers without returning to the original animal basis or checking whether the endpoint is melatonin, circadian output, immune signaling, or a telomere-related marker. By that stage, convention starts to look like evidence.
| Protocol Type | Dosage Range | Administration | Cycle Duration | Primary Research Target |
|---|---|---|---|---|
| Human melatonin trial | 0.5 mg/day | Subcutaneous | Daily dosing used in the reported trial | Melatonin synthesis and circadian regulation |
| Translationally extrapolated framework | 0.5 to 1 mg/day | Subcutaneous | 10 to 20 days, repeated 1 to 2 times annually | Telomere-related and circadian experiments built closer to animal scaling |
| Community longevity protocol | 5 to 10 mg/day | Subcutaneous | 10 to 20 days per cycle, often 1 to 2 cycles per year | Longevity-oriented exploratory research |
| Historical related-compound framework in Russia | 5 to 10 mg/day IM, with intranasal use also reported | Intramuscular or intranasal | 10 to 20 days | Menopause, hormone-related contexts, and related clinical use of Epitalamin |
The practical gap is simple. 0.5 to 1 mg/day is the range that fits the translational logic from the original animal literature. 5 to 10 mg/day is the range that dominates community use. Researchers should treat that as a real methodological fork, not a rounding error.
Higher exposure may still be reasonable in some exploratory work. If the objective is broad phenotypic screening, replication of a legacy protocol, or stress-testing whether any signal appears under a known community schedule, a 5 to 10 mg arm can be justified. The cost is interpretability. Once the dose is many times higher than the translated biological equivalent, it becomes harder to tell whether the observed effect reflects normal pathway engagement, off-target activity, or simple saturation.
For mechanism-focused studies, I would not start at the inherited high range unless there is a specific reason tied to the endpoint. If the hypothesis concerns circadian signaling, pineal effects, or threshold-sensitive biology, the lower range is usually the better first pass. It reduces exposure, improves dose discrimination, and gives the experiment a fair chance to identify a minimum effective level.
A defensible framework looks like this:
The strongest Epitalon protocol is not the highest one. It is the one that matches the biological question, uses high-purity material, controls preparation and route, and makes it possible for another lab to reproduce the result.
Many dosing errors don't start at injection. They start at the bench. A lab can choose the right protocol and still ruin the experiment with poor reconstitution, bad calculations, or rough handling of a fragile lyophilized peptide.
Use a sterile workflow. Start with the lyophilized vial, a sterile syringe, a sterile diluent, alcohol wipes, and a labeling system that records concentration, date, and lot identity. Bacteriostatic Water is the common lab choice because it supports repeated withdrawals after reconstitution.
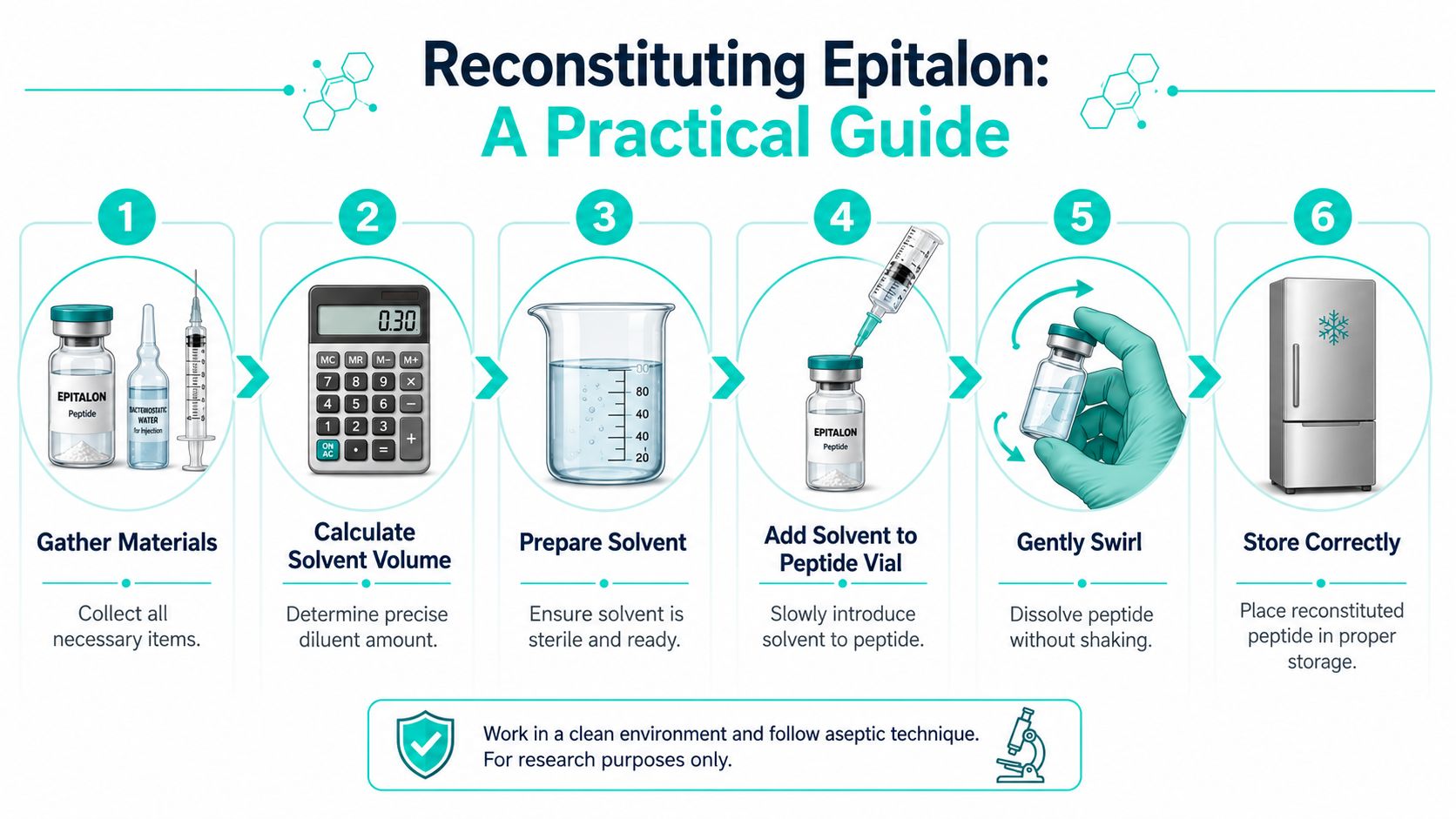
The handling rule is simple. Add the diluent slowly against the glass wall of the vial. Don't blast the powder directly. Once the diluent is in, let the cake dissolve and gently roll or swirl the vial if needed. Don't shake it.
Lab note: Vigorous shaking doesn't make a peptide solution better. It just gives you a faster way to damage what you paid for.
Use this formula every time:
Concentration = total peptide in vial ÷ total diluent added
Then convert that concentration into the volume needed for each planned dose:
Dose volume = target dose ÷ concentration
That calculation prevents the most common mistake in Epitalon work, which is confusing vial size with per-dose amount.
For researchers who want a visual walkthrough before writing the SOP, this brief lab demonstration is useful context:
Suppose the vial contains 10 mg of lyophilized Epitalon. If you add enough diluent to make a final concentration of 1 mg per 0.1 mL, the arithmetic is straightforward:
Under that setup:
That single example shows why reconstitution matters so much in epitalon peptide dosage work. A researcher running a 0.5 mg threshold study and another running a 5 mg replication can use the same vial stock, but only if the concentration is calculated and labeled correctly.
A few practical safeguards reduce errors:
A bad solution can't produce a good dataset.
Route selection changes how much confidence you can place in the dose. With peptides, the nominal dose and the delivered dose aren't always the same thing.

For Epitalon, subcutaneous administration is the most defensible default in modern experimental design. It aligns directly with the human melatonin trial discussed earlier, and it avoids the major absorption problems associated with oral delivery. If a lab wants route consistency, protocol simplicity, and cleaner interpretation, subcutaneous dosing is usually the best choice.
Intramuscular administration has historical precedent, especially in Russian work involving related compounds. It can still be a legitimate route in protocol replication studies, particularly when a researcher is trying to track historical methods rather than optimize convenience.
Intranasal delivery is more situational. Historical use of related compounds includes intranasal ranges, and researchers sometimes consider it when central nervous system access or noninvasive delivery is part of the design question. The trade-off is variability. Nasal absorption is harder to standardize across subjects and setups, so the route can add noise unless the study is built to measure it.
This part is less ambiguous. Oral Epitalon is a weak option for serious research because the peptide has poor oral bioavailability due to enzymatic degradation in the gut, a limitation noted in the human trial summary (oral bioavailability limitation in the trial discussion). If the goal is to study the peptide rather than the failure of a delivery route, oral administration works against the experiment.
A practical comparison helps:
Use the route that removes uncertainty, not the route that sounds easiest in a protocol summary.
Researchers also need to keep route and cycle linked. A short intermittent subcutaneous cycle is not equivalent to a loosely defined noninvasive protocol. If the route changes, the study model changes with it.
A peptide protocol can fail subtly. The vial looks normal, the math is correct, the injections happen on schedule, and the data still drifts because the material degraded or handling standards slipped. Stability isn't glamorous, but it's where reproducibility lives.
Store lyophilized Epitalon in a freezer for long-term preservation. Store the reconstituted solution in a refrigerator for short-term use. Protect both from unnecessary heat, repeated temperature swings, and avoidable light exposure.
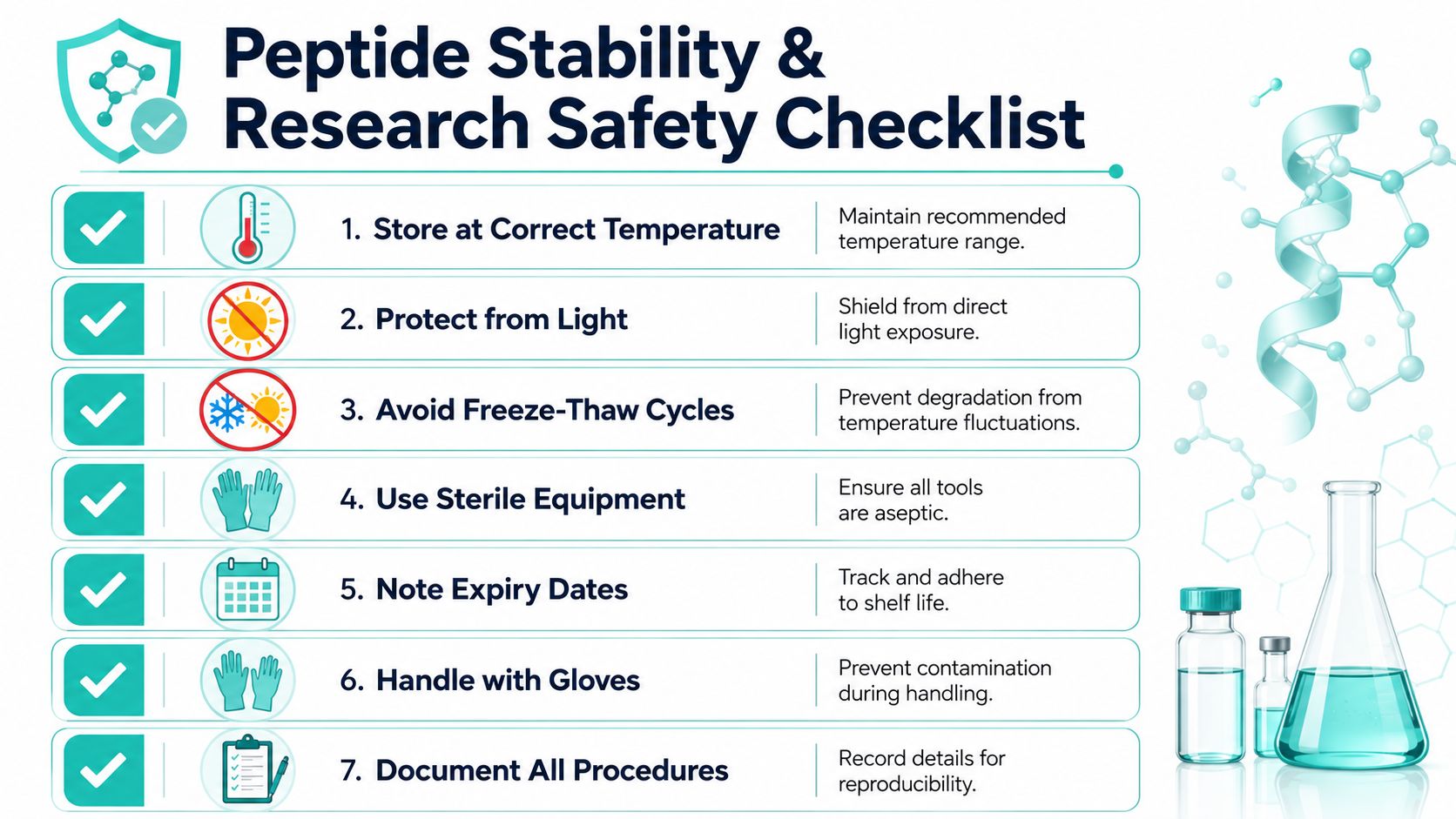
The exact shelf life of a given vial depends on the material, the diluent, the storage consistency, and the lab's own validation rules. What matters operationally is consistency. If one batch spends hours at room temperature and another doesn't, you've introduced a variable before the experiment even begins.
Safety in Epitalon research isn't only about operator protection. It's also about protecting the validity of the study.
Use this checklist:
Good peptide work looks repetitive on paper. That's exactly why it holds up.
One more point deserves blunt wording. Epitalon is sold and discussed as a research compound, not as a dietary supplement or a generally approved therapeutic. That means labs should treat every protocol choice, especially dose escalation, as experimental. The more uncertain the evidence base, the less room there is for casual handling.
No. The published discrepancy is the central issue in this field. The common 5 to 10 mg/day framework may be useful for replication of community protocols, but the translational analysis suggests that 0.5 to 1 mg/day may sit closer to the biologically equivalent human range. More exposure doesn't automatically mean more useful signaling.
The literature commonly clusters around 10 to 20 days of administration, followed by an extended off-period. Some protocols repeat 1 to 2 times per year, and one published commercial-style regimen includes a 4-month break between cycles. For experimental design, intermittent dosing is much easier to justify than continuous use.
It can, but combination studies get complicated fast. If you combine peptides, you won't know which variable produced the effect unless the study is designed around that interaction. For most labs, single-agent dosing is the cleaner first step.
Using the wrong dose for the wrong endpoint. A pineal-focused threshold study shouldn't automatically inherit a high-dose longevity protocol. Route confusion and sloppy reconstitution are close behind.
Think in terms of minimum effective exposure, not maximum tolerated enthusiasm. That mindset usually produces cleaner data and fewer avoidable confounders.
Celonyx Labs supports laboratories and investigators that need research peptides backed by stated 99% purity and independent third-party testing. If your team is building tighter peptide protocols and wants sourcing that fits reproducibility-focused work, review the catalog and quality information at Celonyx Labs.
Stop guessing your peptide doses. Use our free peptide calculator to convert mg, mcg, and
The most surprising fact about Retatrutide isn't that it causes large weight loss. It's that
You're probably in one of two situations right now. Either you've found a peptide you