

Peptide Calculator: Accurate Dosing Tool for Research in 2026
Stop guessing your peptide doses. Use our free peptide calculator to convert mg, mcg, and
The most surprising fact about Retatrutide isn't that it causes large weight loss. It's that the highest-dose arm in a key Phase 3 trial averaged 70.3 lbs lost over 80 weeks, and nearly half of participants crossed the ≥30% weight loss threshold that's clinically associated with bariatric surgery outcomes, according to Lilly's TRIUMPH-1 announcement. For researchers, that moves Retatrutide out of the “next GLP-1 analog” category and into a different class of metabolic tool.
That distinction matters in practice. If a compound combines strong appetite effects with a measurable energy-expenditure component and broad metabolic shifts, then experimental design has to tighten accordingly. Dosing logic, endpoint selection, liver-fat assessment, glycemic tracking, and even procurement standards become more important because poor-quality material can obscure mechanism-driven effects that should be detectable in a clean system.
A useful Retatrutide benefits and analysis discussion has to go beyond benefit lists. The compound's value isn't only in the topline outcomes. It's in the link between triple-receptor pharmacology, system-wide metabolic changes, and the quality controls required to study it correctly.
Retatrutide stands out because it isn't built around a single metabolic lever. It targets GLP-1, GIP, and glucagon receptors together, which gives it a broader physiological footprint than earlier incretin-based approaches. In research terms, that means you're not just studying satiety signaling or glycemic improvement in isolation. You're studying a coordinated intervention that appears to alter appetite, glucose handling, lipid metabolism, and energy expenditure at the same time.
That difference is easy to underestimate if you group Retatrutide with compounds that came before it. A single-agonist GLP-1 framework is useful for appetite suppression and glucose control. A dual-agonist design extends that logic. A triple-agonist design asks a more ambitious question: what happens when the system is pushed through multiple complementary pathways rather than one dominant one?
For investigators, the practical implication is straightforward. Retatrutide is best approached as a systems-metabolism peptide, not just a weight-loss peptide. If your protocol only tracks body weight, you'll miss much of what makes the molecule interesting. Better study designs usually include body composition, glycemic markers, liver-fat endpoints, and cardiometabolic readouts because the mechanism suggests changes should appear across several domains rather than in one isolated outcome.
Practical rule: If the mechanism is multi-axis, your endpoint strategy should be multi-axis too.
That's also why sourcing standards matter more than many teams assume. When the expected signal spans several metabolic endpoints, contaminated or poorly characterized material doesn't just weaken one result. It can blur the entire interpretation of the study.
The cleanest way to understand Retatrutide is to think of it as a three-part orchestra with one conductor. Each receptor pathway contributes a distinct function, but the research value comes from how they work together rather than separately.
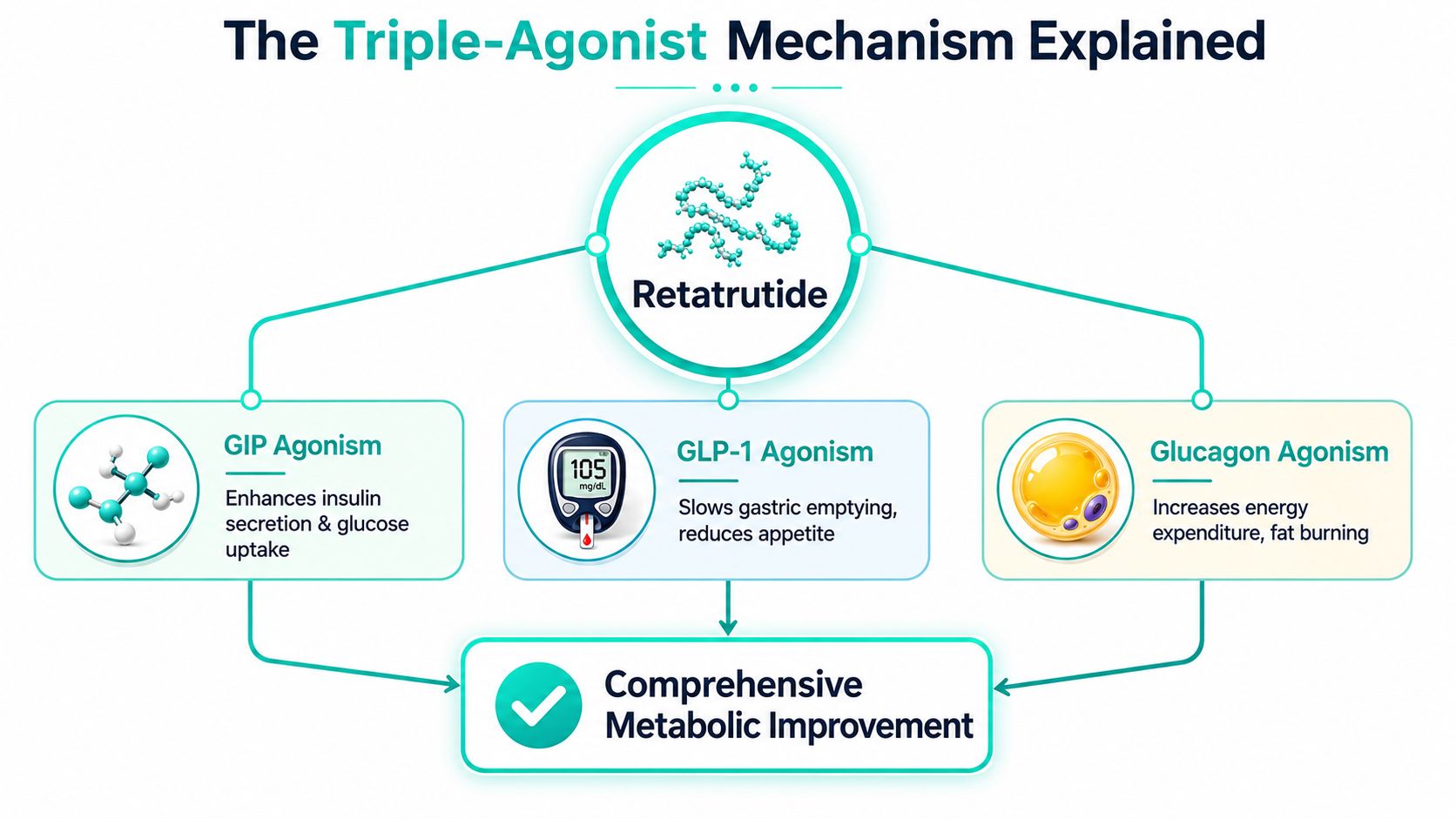
The GLP-1 component is familiar to most metabolic researchers. It supports appetite reduction and slows gastric emptying, which can lower caloric intake and flatten postprandial glucose excursions. That alone can produce meaningful changes in metabolic models.
The GIP component adds another layer. In practical terms, it complements insulin-related signaling and glucose uptake. In combination with GLP-1 agonism, it contributes to a stronger metabolic response than single-pathway appetite suppression would usually produce on its own.
These two pathways often get most of the attention because they map neatly onto satiety and glycemic control. But Retatrutide's distinctive profile doesn't stop there.
The glucagon receptor arm is where Retatrutide becomes more than an incretin extension. This pathway is associated with increased energy expenditure and fat mobilization. That matters because a peptide that reduces intake is one thing. A peptide that reduces intake while also shifting energy use is a different experimental entity.
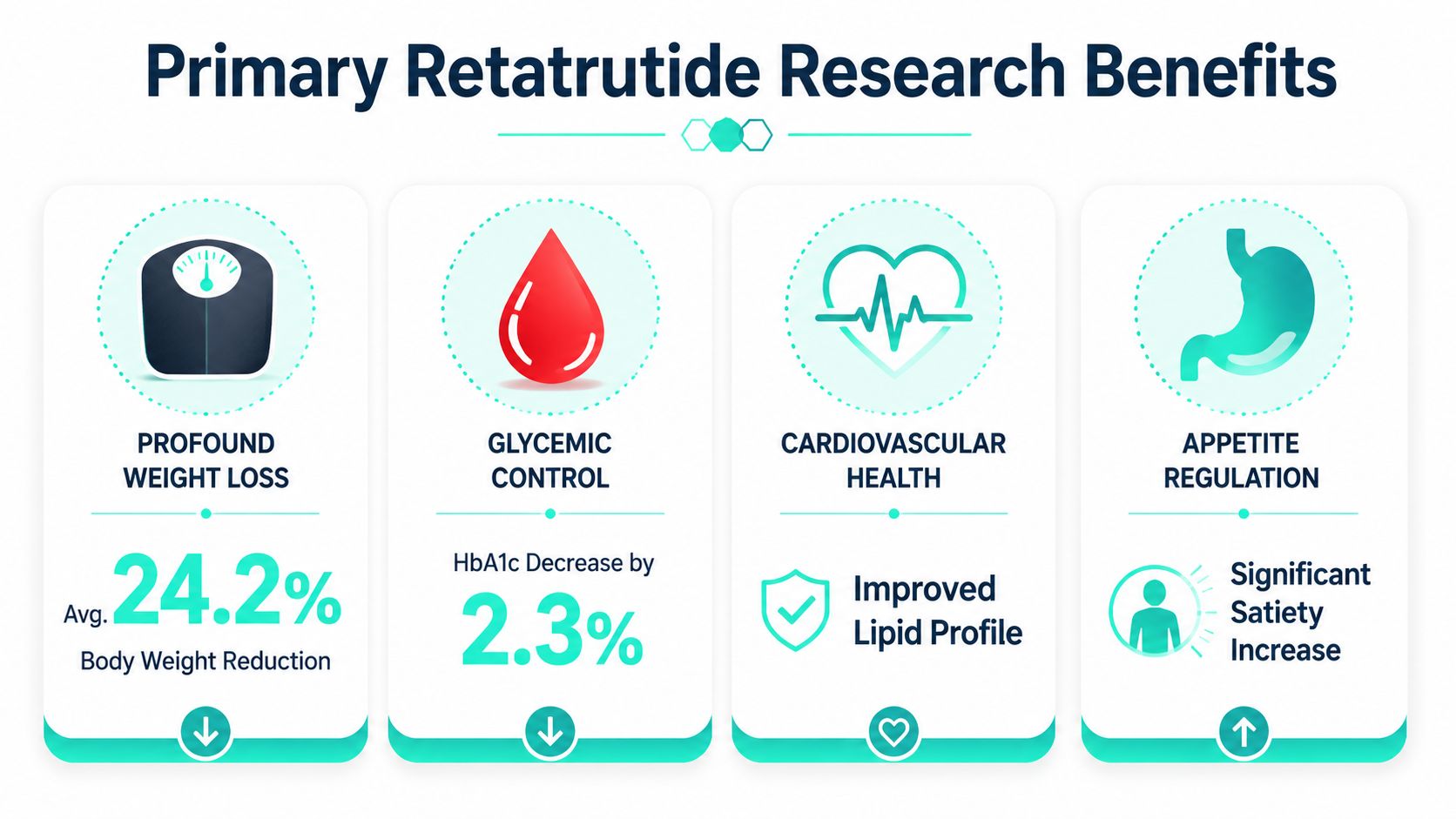
A summary of Phase 2 findings describes Retatrutide as a novel triple receptor agonist acting on GLP-1, GIP, and glucagon pathways, with the 12 mg weekly dose achieving a mean 24.2% body weight reduction at 48 weeks, with 100% of participants on 8 mg or 12 mg reaching ≥5% weight loss, while also reducing liver fat by more than 80% in high-dose cohorts. Mechanistically, that combination is consistent with a model in which glucagon-mediated hepatic lipolysis contributes to the broader metabolic shift.
The peptide's significance isn't that it hits three receptors. It's that those three receptors point in a compatible metabolic direction.
Single-agonist studies can sometimes isolate a dominant effect and treat everything else as a secondary consequence. Retatrutide doesn't fit that pattern cleanly. When appetite suppression, insulin-related signaling, and energy expenditure all move together, observed outcomes may reflect synergy rather than simple additivity.
That has a few direct consequences for researchers:
A good Retatrutide benefits and analysis framework starts here. If you miss the mechanism, the clinical outcomes look impressive but disconnected. Once you understand the mechanism, the outcomes look internally coherent.
Retatrutide matters because its primary outcomes line up cleanly with its receptor biology. The practical value is not a vague promise of broad metabolic activity. It is a repeatable pattern across weight, glycemia, and liver fat that researchers can tie back to a triple-agonist design and then use to build better studies and stricter sourcing criteria.
The body-weight signal is large enough to change how comparator work should be framed. In Lilly's report on the TRIUMPH-1 Phase 3 trial, the highest dose produced substantial weight reduction over an extended observation period.
Key figures from that report explain why the peptide is attracting so much attention:
| Outcome | Reported finding |
|---|---|
| Average weight loss at 12 mg over 80 weeks | 70.3 lbs (28.3%) |
| Participants reaching ≥30% weight loss | 45.3% |
| Participants reaching BMI below 30 | 65.3% |
| Participants with baseline class 3 obesity who reached BMI below 30 | 37.5% |
| Average weight reduction at 104 weeks in the blinded extension for baseline BMI ≥35 | 85.0 lbs (30.3%) |
Those numbers have direct experimental implications. A short study window can misread the phenotype by capturing early appetite effects while missing later consolidation in body composition and metabolic markers. Teams selecting endpoints at 8 to 16 weeks should be careful about making ranking claims against GLP-1-only comparators if the mechanism suggests a longer response curve.
I usually treat this as a protocol problem before I treat it as a pharmacology problem. If the expected effect size is large but the study duration, dosing schedule, or peptide quality is weak, the result is not a clean negative. It is an uninterpretable study.
The stakeholder summary often pulled from conference discussion is straightforward. The weight-loss effect appears deep, sustained, and still developing late in follow-up. That point is more useful than any embedded commentary video because it affects how washout periods, interim analyses, and responder thresholds should be set.
Weight loss alone does not explain the interest in Retatrutide. Earlier company-reported trial results also described strong glycemic improvement in participants with type 2 diabetes, including movement of A1C into ranges associated with tighter glucose control, with continued improvement through the reported observation window as noted earlier.
For researchers, this changes model selection. Retatrutide is poorly matched to narrow obesity-only systems if the underlying question involves adiposity plus impaired glucose handling. A model that captures both gives a more faithful readout of the compound's phenotype.
It also changes assay priorities. Fasting glucose, A1C, insulin-related markers, and feeding behavior should be planned together rather than split into primary and convenience endpoints. If those readouts separate across lots, dose groups, or suppliers, that inconsistency can be an early warning that the material, not the biology, is the source of the problem.
Lab note: If a lot produces appetite suppression without the expected glucose-side signal, I would verify identity, purity profile, and reconstitution history before drawing mechanistic conclusions.
The hepatic signal is one of the most practical reasons to take Retatrutide seriously in translational work. Earlier reported clinical findings described marked relative reductions in liver fat at higher doses, which places the peptide in a different category from compounds studied only for body-mass change.
That matters because liver-fat endpoints are less forgiving of poor material quality and weak study control. If a peptide lot is partially degraded, improperly stored, or inconsistently dosed, investigators may still see some effect on intake while losing a cleaner integrated hepatic response. That kind of partial phenotype can send a team toward the wrong mechanistic explanation.
Three design decisions follow from that risk:
That is the practical center of a serious Retatrutide analysis. The primary benefits are coherent because the mechanism is coherent. Researchers who want valid data need to connect those outcome domains to study length, endpoint selection, and peptide source quality from the start.
Retatrutide is more than a weight-loss signal. The triple-agonist profile makes that point clear. When a compound changes appetite, glycemic control, energy expenditure, and body composition at the same time, researchers should expect secondary phenotypes across cardiovascular, inflammatory, respiratory, and functional domains.

The practical question is not whether downstream effects exist. The question is which of them reflect direct biology and which are largely consequences of reduced adiposity.
Earlier clinical reporting described favorable movement in waist circumference, lipids, inflammatory markers, and blood pressure. That pattern fits the mechanism. GLP-1 activity can improve glycemic control and reduce intake. GIP signaling may influence insulin dynamics and adipose handling. Glucagon receptor agonism appears to contribute to energy expenditure and hepatic metabolic effects, while also increasing the need for careful dose interpretation because tolerability and catabolic stress can shift with exposure.
That mechanistic mix matters for study design. If several cardiometabolic markers improve together, the result should not be treated as a generic halo effect. It may indicate that the intervention is altering multiple linked systems at once, which is exactly why poor reagent quality or unstable material can produce confusing partial phenotypes. A study might still show body-mass change while underreporting effects on inflammation, glucose regulation, or cardiovascular readouts.
Secondary observations reported in broader coverage also point to possible effects on body fat distribution, sleep-disordered breathing, and weight-linked pain outcomes, including a UCHealth summary. Those findings are useful for hypothesis generation, but they should be ranked below primary endpoint data unless the protocol was built to test them directly.
Researchers get cleaner answers when they define the expected causal chain before the first dose is prepared.
For cardiometabolic studies, pair scale weight with waist measures, fasting glucose, HbA1c, lipids, blood pressure, and an inflammatory marker panel. That setup helps distinguish a broad metabolic response from a narrower weight-driven effect. If only anthropometric measures move, the interpretation is different from a dataset where glycemia, lipids, and inflammation shift in parallel.
Musculoskeletal and sleep outcomes need even more restraint. Reduced joint pain can reflect lower mechanical loading, lower inflammatory tone, altered activity, or some combination of the three. Fewer apnea events may follow from changes in neck circumference, visceral fat, ventilatory control, or overall metabolic status. Those are related hypotheses, not interchangeable ones.
A useful framework is simple:
The standard for evidence should rise as the claim gets broader.
Retatrutide is most interesting in this section not because it produces a long list of favorable outcomes, but because its triple-agonist mechanism provides a plausible route to those outcomes. Serious analysis connects that biology to endpoint selection, timing, and material control. Without that connection, secondary effects are easy to overread and hard to reproduce.
A Retatrutide experiment is only as trustworthy as the material placed into it. Researchers often spend weeks refining protocol logic and endpoint selection, then accept weak sourcing documents that would never pass scrutiny if they were attached to a critical reagent or analytical standard. That's a mistake.
Low-grade peptide material creates noise in at least three ways. It can alter apparent potency, introduce off-target biological effects, and destabilize batch-to-batch interpretation. When the expected phenotype includes changes in appetite-related behavior, glycemic markers, and hepatic outcomes, any impurity problem can distort multiple endpoints at once.

Third-party verification only matters if it's real and checkable. According to guidance on independently verified research peptides, a credible Certificate of Analysis must explicitly name the laboratory, and that lab should have a discoverable web presence, published methodology, and accreditation list. If the lab is unnamed or can't be independently verified, the claim fails basic credibility.
That standard is practical, not cosmetic. An unnamed lab can't be audited by the buyer. A vague purity claim without lot-specific analytical context doesn't tell you whether the material in hand matches the document provided.
Researchers should also understand the role of third-party testing at a broader level. Independent testing is meant to verify identity, screen for contaminants, assess residual solvents, and quantify problematic aggregates. In other words, the external lab acts as an objective check rather than an internal marketing extension.
When reviewing Retatrutide procurement, I'd want a supplier to satisfy the following before any long-duration study starts:
A more stringent quality mindset is justified for Retatrutide because the compound's expected effects are complex enough that poor sourcing can easily produce false negatives, partial positives, or misleading comparisons.
Procurement test: If a supplier's quality story depends more on branding language than on verifiable documents, keep looking.
Even high-quality peptide material can be compromised after delivery. Labs sometimes focus heavily on supplier selection and then lose control during receipt, reconstitution, or repeated access in routine use. With a research peptide like Retatrutide, handling discipline protects both stability and interpretability.
Start with documentation, not the vial cap. On arrival, confirm that the received lot matches the purchase record and associated COA. Check labeling, container integrity, and shipping condition immediately. If anything is unclear, quarantine the batch until the discrepancy is resolved.
For lyophilized material, the basic principle is simple. Keep the peptide dry, protected from avoidable temperature stress, and exposed to as little environmental fluctuation as possible. Repeated warming and cooling cycles, unnecessary light exposure, and poor inventory control all increase the risk of degradation or confusion.
A practical intake workflow usually includes:
Once a peptide is reconstituted, the risk profile changes. Liquid preparations are generally more vulnerable than lyophilized stock, so the best practice is to reconstitute only what the protocol needs over a practical working window.
Use a solvent appropriate to your laboratory protocol and compatibility requirements. Many labs use bacteriostatic water or another validated diluent depending on the intended research application. Add the solvent gently rather than forcing a high-pressure stream directly onto the peptide cake. Swirling is usually preferable to aggressive shaking because harsh mechanical handling can damage delicate material.
For daily handling, the priorities are consistency and contamination control:
Storage temperatures and hold times should follow the supplier's validated guidance for the specific formulation and packaging provided. Without lot-specific instructions, the right answer is caution, not assumption. Researchers sometimes borrow storage rules from unrelated peptides. That's convenient, but it isn't good science.
Retatrutide belongs in a different planning category than single-pathway incretin peptides. Its combined GLP-1, GIP, and glucagon receptor activity can shift appetite, glycemic control, energy expenditure, and other metabolic readouts at the same time. For researchers, that means the peptide itself and the procurement workflow both need tighter control if the goal is interpretable data.
Retatrutide is better understood as a multi-receptor metabolic tool. GLP-1 signaling explains only part of the observed effect profile. GIP and glucagon receptor engagement matter because they can change how a study reads out across body weight, glucose handling, and broader cardiometabolic markers.
That wider mechanism has a practical consequence. Study designs built around a single expected endpoint can miss signal, or misread noise as a treatment effect.
Independent verification reduces a basic procurement problem. A supplier cannot objectively validate its own material without conflict. According to an explanation of third-party peptide testing, external testing can confirm sequence identity and check for contaminants, residual solvents, and aggregation.
In practice, the documentation matters as much as the claim. If a supplier says a batch was tested by a third party but cannot provide lot-linked records from a named laboratory, the statement does not help much during study review or deviation analysis.
Start with continuity and traceability. Retatrutide studies often run long enough that a weak procurement plan becomes a data problem.
Before the first dosing day, labs should confirm the following:
This step is often underestimated. A clean protocol cannot rescue poorly documented material.
Generic certificates are a problem. Missing lot numbers, vague purity language, unnamed testing labs, and records that cannot be tied to the exact vial on hand all increase risk.
I also treat weak answers on shipping conditions, storage controls, and deviation handling as procurement warnings. If a supplier cannot explain how material integrity is protected before it reaches the lab, the biological results become harder to trust.
Research-grade Retatrutide is laboratory material. It is not an approved clinical product, and it should not be represented that way in procurement records, internal communication, or study governance.
That distinction protects both compliance and data quality. Teams make avoidable mistakes when they borrow assumptions from clinical supply chains that do not apply to research procurement.
Batch consistency matters because the expected phenotype is broad. With a narrower compound, lot variation may distort one primary readout. With Retatrutide, inconsistency can affect body weight, glycemic measures, and secondary metabolic outcomes in parallel, which makes root-cause analysis harder after the fact.
For that reason, quality sourcing is part of experimental design, not an administrative task handled after the protocol is written.
Researchers who need dependable peptide sourcing should prioritize suppliers with clear quality standards, accessible batch documentation, and procurement practices built for repeatable lab work. Celonyx Labs supports that model with a laboratory peptide catalog, stated purity standards, and independent third-party testing that can help reduce avoidable variability before a study begins.
Stop guessing your peptide doses. Use our free peptide calculator to convert mg, mcg, and
The most surprising fact about Retatrutide isn't that it causes large weight loss. It's that
You're probably in one of two situations right now. Either you've found a peptide you